
Etiology Model for Kawasaki Disease, Multisystem Inflammatory Syndrome (MIS) in Children (MIS-C), adults (MIS-A), neonates (MIS-N), and after vaccination (MIS-V)
Etiology Model for Kawasaki Disease, Multisystem Inflammatory Syndrome (MIS) in Children (MIS-C), adults (MIS-A), neonates (MIS-N), and after vaccination (MIS-V)
Immune complexes activating Fc receptors on immune cells and platelets model

Kawasaki disease (KD) or mucocutaneous lymph node syndrome and Multisystem Inflammatory Syndromes (MIS) are associated with inflammation of medium-sized blood vessels (vasculitis). KD was first described in 1965 and still has unknown disease etiology. It is a rare disease that mostly affects children under the age of 5 years old. Some KD children can develop coronary artery aneurysms (CAA) or lesions (CAL); KD is a leading cause of heart disease in children.
With the COVID-19 outbreak, diseases similar to KD appeared in children (MIS-C), adults (MIS-A), neonates (MIS-N), and after COVID-19 vaccination (MIS-V). The medical community considers these to be distinct diseases from KD. There is a lot of overlaps in symptoms, with MIS-C also affecting children older than 5 years of age. Ventrical dysfunction appears with MIS-X patients.
Published: Ricke, D.O.; Smith, N. VAERS Vasculitis Adverse Events Retrospective Study: Etiology Model of Immune Complexes Activating Fc Receptors in Kawasaki Disease and Multisystem Inflammatory Syndromes. Life 2024, 14, 353. https://doi.org/10.3390/life14030353
Hypothesis 1: The etiology of Kawasaki Disease remains unknown and there is no association between Kawasaki Disease and vaccination. Note: the medical community continues to search for the pathogen that causes KD. A subset of the medical community do consider that KD might be associated immune disregulation. [The following data should refute: (1) that KD has a single causative agent with support for (2) KD cases can be caused by a variety of pathogens or a variety of vaccines].
Hypothesis 2: Kawasaki Disease (and also MIS-X diseases) are caused by immune complexes from either persistent infections or immunization activating immune cells and platelets with risk level increased by relevant genetic variants.
Multiple clinical studies have attempted to identify a causative infectious agent for KD. Clusters of KD cases frequently occur with a 4 to 6 week onset delay following pathogen outbreaks. Associations between KD and multiple pathogens have been reported:
· adenovirus[5,6],
· human bocavirus[7],
· coronavirus[6],
· human coronavirus 229E[8],
· human coronavirus (HCoV-NH) NL63[9],
· cytomegalovirus[10],
· dengue[11,12],
· enterovirus[6,13],
· Epstein–Barr virus[14],
· human herpesvirus 6[15],
· human lymphotropic virus[16],
· human rhinovirus[6],
· influenza[17],
· measles[18],
· parvovirus B19[19,20],
· parainfluenza virus type 2[21],
· respiratory syncytial virus (RSV)[22],
· rotavirus[23],
· varicella zoster (chicken pox)[24,25],
· torque teno virus[26],
· Staphylococcus aureus[27], and
· Streptococcus[14,28].
KD has also been reported as a rare adverse event associated with vaccinations and vaccine combinations:
· Bacillus Calmette-Gue’rin (BCG) vaccination [29],
· COVID-19 vaccine Vaxzevria (nonreplicating viral vector)[30],
· Diphtheria, tetanus, and acellular pertussis (DTaP or DTAP) [31],
· Hepatitis b [32],
· Influenza [31,33-35],
· Lanzhou lamb rotavirus vaccine (LLR) and freeze-dried live attenuated hepatitis A vaccine (HAV or HEPA)[36],
· Measles, mumps, and rubella (MMR) [31],
· Polysaccharide pneumococcal vaccine (Pneumo 23) [34],
· Pneumococcal conjugate vaccine (PCV or PNC) [31],
· Rotavirus [31,37],
· SARS-CoV-2 [38],
· Yellow fever vaccine [39],
· DTaP/Poliovirus vaccine inactivated (IPV)/ Hepatitis B virus vaccine (HepB or HEP), [40];
· Prevnar 13 (PNC13 or PCV13)
· Rotarix [40],
· DTaP/IPV/Haemophilus B conjugate vaccine (Hib or HIBV)/PCV [41],
· DTaP/IPV/Hib; meningitis C; PCV [41],
· DTaP/IPV; MMR [41],
· DTaP-IPV/Hib and PCV13 [42],
· Hib; meningitis C; PCV; MMR [41],
· Measles/rubella (MR), varicella, pneumococcal [43].
· One report of an adult with both KD and (MIS-A) following second dose of Pfizer SARS-CoV-2 vaccine [38].
This establishes that KD has been reported associated with multiple pathogens (including two bacterial pathogens) and also multiple vaccines. The key is that antibody responses to these pathogens or vaccines have antibody heavy chain segments that can bind to Fc antibody receptors on immune cells and platlets. If the concentration of antibodies is high enough, KD or MIS-X can be triggered. Fc receptors typically have low affinity for IgG antibodies (hence the requirement for higher antibody titer levels to drive the disease process). A persistent infection (e.g., an gastrointestinal SARS-CoV-2 infection could drive MIS-C, etc.) is one method of driving antibody titers higher than primary immune response levels. The high antibody titer requirement likely accounts for the delay of onset for both KD and MIS-X after pathogen outbreaks by roughly 4 to 6 weeks.
The United States HHS.gov supports the Vaccine Adverse Event Reporting System (VAERS) for all adverse events reported after immunizations. This is a passive reporting system the collects only a very small subset of all of the adverse events. Examining the VAERS database, it should be possible to see possible associations between vaccines and either KD or MIS. To normalize the adverse events reported, they are divided by the total number of reports to VAERS for each vaccine and multiplied by 100,000; the computed frequency is the expected frequency per 100,000 adverse event reports.
Table 1. Kawasaki Disease adverse event reports with normalized frequency per 100,000 patients with reported symptoms in VAERS; data from 1990 until October 27, 2023. A subset of vaccines are illustrated.
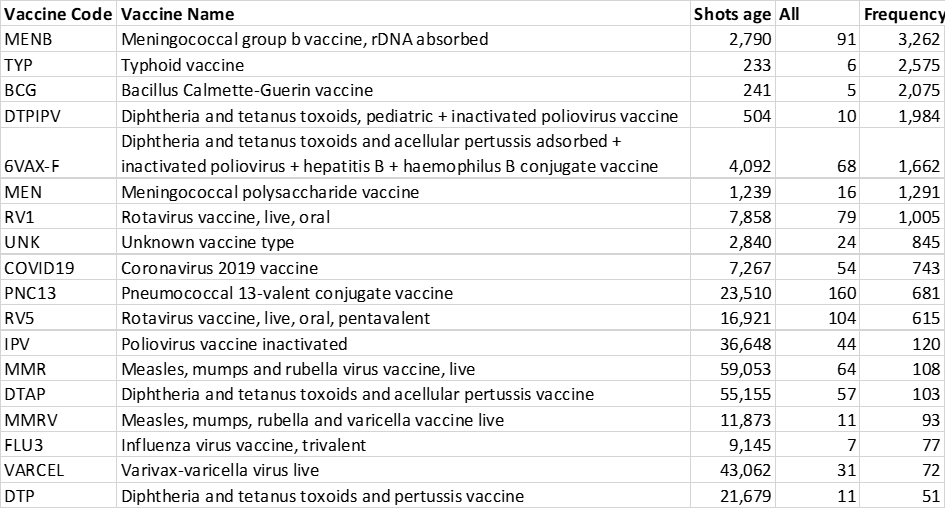
The normalized frequencies in Table 1 can not represent normal background chance associations. Some vaccines appear to trigger KD at higher frequencies than other vaccines. It would be worth investigating possible manufacturing contaminants (e.g., endotoxins - see posts by Dr. Geoff Pain (Example)).
The disease symptoms for KD and MIS combined with disease characteristics, associations with multiple pathogens, associations with multiple vaccines, and unusual treatments points towards a candidate etiology of immune complexes activating immune cells and platelets via Fc receptor binding resulting in release of inflammatory molecules including histamine and serotonin. This model proposes that antibody levels higher than primary immune response levels binding to either infectious pathogen or vaccine protein creating immune complexes are circulating and activating immune responses by binding to Fc receptors on immune cells and platelets including granulocytes and mast cells. Vasculitis, rash, and fever are associated with Type III hypersensitivity-like responses to immune complexes. Activation of platelets and likely granulocytes including mast cells induce release of high levels of histamine, serotonin, and other inflammatory molecules associated with mast cell activation syndrome (MCAS) symptoms, including fever, rash, diarrhea, nausea, vomiting, red eyes, headaches, migraines, palpitation, arrhythmia, etc. Elevated levels of serotonin are associated with vasoconstrictions. Contraction of cardiac capillary pericyte cells in response to high levels of histamine has been previously proposed to cause (pressure induced) coronary artery aneurysms, myocarditis, pericarditis. Pericytes, attached to the surface of capillaries, play an important role in local blood flow. Pericytes are also involved in innate immune responses. Pericytes also mediate coronary no-reflow after myocardial ischemia. Immune responses to infectious pathogens are likely associated with overlapping symptoms.
See also: Ricke DO, Gherlone N, Fremont-Smith P, Tisdall P, Fremont-Smith M. Kawasaki Disease, Multisystem Inflammatory Syndrome in Children: Antibody-Induced Mast Cell Activation Hypothesis. J Pediatrics & Pediatr Med. 2020; 4(2): 1-7 article
References
5. Embil, J.A.; McFarlane, E.S.; Murphy, D.M.; Krause, V.W.; Stewart, H.B. Adenovirus type 2 isolated from a patient with fatal Kawasaki disease. Can Med Assoc J 1985, 132, 1400-1400.
6. Chang, L.-Y.; Lu, C.-Y.; Shao, P.-L.; Lee, P.-I.; Lin, M.-T.; Fan, T.-Y.; Cheng, A.-L.; Lee, W.-L.; Hu, J.-J.; Yeh, S.-J.; et al. Viral infections associated with Kawasaki disease. J Formos Med Assoc 2014, 113, 148-154, doi:10.1016/j.jfma.2013.12.008.
7. Catalano-Pons, C.; Giraud, C.; Rozenberg, F.; Meritet, J.F.; Lebon, P.; Gendrel, D. Detection of human bocavirus in children with Kawasaki disease. Clin Microbiol Infect 2007, 13, 1220-1222, doi:https://doi.org/10.1111/j.1469-0691.2007.01827.x.
8. Shirato, K.; Imada, Y.; Kawase, M.; Nakagaki, K.; Matsuyama, S.; Taguchi, F. Possible involvement of infection with human coronavirus 229E, but not NL63, in Kawasaki disease. J Med Virol 2014, 86, 2146-2153, doi:10.1002/jmv.23950.
9. Esper, F.; Weibel, C.; Ferguson, D.; Landry, M.L.; Kahn, J.S. Evidence of a Novel Human Coronavirus That Is Associated with Respiratory Tract Disease in Infants and Young Children. The Journal of Infectious Diseases 2005, 191, 492-498, doi:10.1086/428138.
10. Catalano-Pons, C.; Quartier, P.; Leruez-Ville, M.; Kaguelidou, F.; Gendrel, D.; Lenoir, G.; Casanova, J.-L.; Bonnet, D. Primary Cytomegalovirus Infection, Atypical Kawasaki Disease, and Coronary Aneurysms in 2 Infants. Clin Infect Dis 2005, 41, e53-e56, doi:10.1086/432578.
11. Jagadeesh, A.; Krishnamurthy, S.; Mahadevan, S. Kawasaki Disease in a 2-year-old Child with Dengue Fever. Indian J Pediatr 2016, 83, 602-603, doi:10.1007/s12098-015-1927-8.
12. Sopontammarak, S.; Promphan, W.; Roymanee, S.; Phetpisan, S. Positive Serology for Dengue Viral Infection in Pediatric Patients With Kawasaki Disease in Southern Thailand. Circ J 2008, 72, 1492-1494, doi:10.1253/circj.CJ-08-0158.
13. Weng, K.-P.; Cheng-Chung Wei, J.; Hung, Y.-M.; Huang, S.-H.; Chien, K.-J.; Lin, C.-C.; Huang, S.-M.; Lin, C.-L.; Cheng, M.-F. Enterovirus Infection and Subsequent Risk of Kawasaki Disease: A Population-based Cohort Study. Pediatr Infect Dis J 2018, 37.
14. Kikuta, H.; Nakanishi, M.; Ishikawa, N.; Konno, M.; Matsumoto, S. Detection of Epstein-Barr virus sequences in patients with Kawasaki disease by means of the polymerase chain reaction. Intervirology 1992, 33, 1-5, doi:10.1159/000150224.
15. Okano, M.; Luka, J.; Thiele, G.M.; Sakiyama, Y.; Matsumoto, S.; Purtilo, D.T. Human herpesvirus 6 infection and Kawasaki disease. J Clin Microbiol 1989, 27, 2379-2380.
16. Okano, M. Kawasaki Disease and Human Lymphotropic Virus Infection. Curr Med Res Opin 1999, 15, 129-134, doi:10.1185/03007999909113373.
17. Joshi, A.V.; Jones, K.D.J.; Buckley, A.-M.; Coren, M.E.; Kampmann, B. Kawasaki disease coincident with influenza A H1N1/09 infection. Pediatr Int 2011, 53, e1-e2, doi:10.1111/j.1442-200X.2010.03280.x.
18. Whitby, D.; Hoad, J.G.; Tizard, E.J.; Dillon, M.J.; Weber, J.N.; Weiss, R.A.; Schulz, T.F. Isolation of measles virus from child with Kawasaki disease. Lancet 1991, 338, 1215, doi:https://doi.org/10.1016/0140-6736(91)92085-G.
19. Holm, J.M.; Hansen, L.K.; Oxhøj, H. Kawasaki disease associated with parvovirus B19 infection. Eur J Pediatr 1995, 154, 633-634, doi:10.1007/BF02079066.
20. Nigro, G.; Krzysztofiak, A.; Porcaro, M.A.; Mango, T.; Zerbini, M.; Gentilomi, G.; Musiani, M. Active or recent parvovirus B19 infection in children with Kawasaki disease. Lancet 1994, 343, 1260-1261, doi:https://doi.org/10.1016/S0140-6736(94)92154-7.
21. Keim, D.; Keller, E.; Hirsch, M. Mucocutaneous Lymph-Node Syndrome and Parainfluenza 2 Virus Infection. Lancet 1977, 310, 303, doi:https://doi.org/10.1016/S0140-6736(77)90990-4.
22. Kim, G.B.; Park, S.; Kwon, B.S.; Han, J.W.; Park, Y.W.; Hong, Y.M. Evaluation of the Temporal Association between Kawasaki Disease and Viral Infections in South Korea. Korean Circ J 2014, 44, 250-254, doi:10.4070/kcj.2014.44.4.250.
23. Matsuno, S.; Utagawa, E.; Sugiura, A. Association of Rotavirus Infection with Kawasaki Syndrome. The Journal of Infectious Diseases 1983, 148, 177-177, doi:10.1093/infdis/148.1.177.
24. Ogboli, M.I.; Parslew, R.; Verbov, J.; Smyth, R. Kawasaki disease associated with varicella: a rare association. Br J Dermatol 1999, 141, 1136-1152, doi:10.1046/j.1365-2133.1999.03231.x.
25. Kossiva, L.; Papadopoulos, M.; Lagona, E.; Papadopoulos, G.; Athanassaki, C. Myocardial infarction in a 35-day-old infant with incomplete Kawasaki disease and chicken pox. Cardiol Young 2010, 20, 567-570, doi:10.1017/S1047951109991478.
26. Thissen, J.B.; Isshiki, M.; Jaing, C.; Nagao, Y.; Lebron Aldea, D.; Allen, J.E.; Izui, M.; Slezak, T.R.; Ishida, T.; Sano, T. A novel variant of torque teno virus 7 identified in patients with Kawasaki disease. PLoS One 2018, 13, e0209683-e0209683, doi:10.1371/journal.pone.0209683.
27. Hall, M.; Hoyt, L.; Ferrieri, P.; Schlievert, P.M.; Jenson, H.B. Kawasaki Syndrome-Like Illness Associated with Infection Caused by Enterotoxin B-Secreting Staphylococcus aureus. Clin Infect Dis 1999, 29, 586-589, doi:10.1086/598638.
28. Shinomiya, N.; Takeda, T.; Kuratsuji, T.; Takagi, K.; Kosaka, T.; Tatsuzawa, O.; Tsurumizu, T.; Hashimoto, T.; Kobayashi, N. Variant Streptococcus sanguis as an etiological agent of Kawasaki disease. Prog Clin Biol Res 1987, 250, 571-572.
29. Banday, A.Z.; Patra, P.K.; Jindal, A.K. Kawasaki disease – when Bacillus Calmette–Guérin (BCG) lymphadenitis blooms again and the vaccination site peels off! International Journal of Dermatology 2021, 60, e233-e234, doi:https://doi.org/10.1111/ijd.15348.
30. Peralta-Amaro, A.L.; Tejada-Ruiz, M.I.; Rivera-Alvarado, K.L.; Cobos-Quevedo, O.D.; Romero-Hernández, P.; Macías-Arroyo, W.; Avendaño-Ponce, A.; Hurtado-Díaz, J.; Vera-Lastra, O.; Lucas-Hernández, A. Atypical Kawasaki Disease after COVID-19 Vaccination: A New Form of Adverse Event Following Immunization. Vaccines (Basel) 2022, 10, doi:10.3390/vaccines10010126.
31. Alsager, K.; Khatri Vadlamudi, N.; Jadavji, T.; Bettinger, J.A.; Constantinescu, C.; Vaudry, W.; Tan, B.; Sauvé, L.; Sadarangani, M.; Halperin, S.A.; et al. Kawasaki disease following immunization reported to the Canadian Immunization Monitoring Program ACTive (IMPACT) from 2013 to 2018. Human Vaccines & Immunotherapeutics 2022, 18, 2088215, doi:10.1080/21645515.2022.2088215.
32. Miron, D.; Fink, D.; Hashkes, P.J. Kawasaki disease in an infant following immunisation with hepatitis B vaccine. Clin Rheumatol 2003, 22, 461-463, doi:10.1007/s10067-003-0785-3.
33. Jeong, S.W.; Kim, D.H.; Han, M.Y.; Cha, S.H.; Yoon, K.L. An infant presenting with Kawasaki disease following immunization for influenza: A case report. Biomed Rep 2018, 8, 301-303, doi:10.3892/br.2018.1043.
34. Kraszewska-Głomba, B.; Kuchar, E.; Szenborn, L. Three episodes of Kawasaki disease including one after the Pneumo 23 vaccine in a child with a family history of Kawasaki disease. Journal of the Formosan Medical Association 2016, 115, 885-886, doi:https://doi.org/10.1016/j.jfma.2016.04.005.
35. Shimada, S.; Watanabe, T.; Sato, S. A Patient with Kawasaki Disease Following Influenza Vaccinations. Pediatr Infect Dis J 2015, 34.
36. Yin, S.; Liubao, P.; Chongqing, T.; Xiaomin, W. The first case of Kawasaki disease in a 20-month old baby following immunization with rotavirus vaccine and hepatitis A vaccine in China: A case report. Human Vaccines & Immunotherapeutics 2015, 11, 2740-2743, doi:10.1080/21645515.2015.1050571.
37. Huang, W.-T.; Juan, Y.-C.; Liu, C.-H.; Yang, Y.-Y.; Chan, K.A. Intussusception and Kawasaki disease after rotavirus vaccination in Taiwanese infants. Vaccine 2020, 38, 6299-6303, doi:https://doi.org/10.1016/j.vaccine.2020.07.038.
38. Showers, C.R.; Maurer, J.M.; Khakshour, D.; Shukla, M. Case of adult-onset Kawasaki disease and multisystem inflammatory syndrome following SARS-CoV-2 vaccination. BMJ Case Reports 2022, 15, e249094, doi:10.1136/bcr-2022-249094.
39. Schmöeller, D.; Keiserman, M.W.; Staub, H.L.; Velho, F.P.; de Fátima Grohe, M. Yellow Fever Vaccination and Kawasaki Disease. The Pediatric Infectious Disease Journal 2009, 28.
40. Chang, A.; Islam, S. Kawasaki disease and vasculitis associated with immunization. Pediatrics International 2018, 60, 613-617, doi:https://doi.org/10.1111/ped.13590.
41. Hall, G.C.; Tulloh, R.M.R.; Tulloh, L.E. The incidence of Kawasaki disease after vaccination within the UK pre-school National Immunisation Programme: an observational THIN database study. Pharmacoepidemiology and Drug Safety 2016, 25, 1331-1336, doi:https://doi.org/10.1002/pds.4108.
42. Ece, I.; Akbayram, S.; Demiroren, K.; Uner, A. Is Kawasaki Disease a Side Effect of Vaccination as Well? J Vaccines Vaccin 2014, 5, doi:10.4172/2157-7560.1000234.
43. Matsubara, D.; Minami, T.; Seki, M.; Tamura, D.; Yamagata, T. Occurrence of Kawasaki disease after simultaneous immunization. Pediatrics International 2019, 61, 1171-1173, doi:https://doi.org/10.1111/ped.13965.
The US Government Comparative Toxicogenomics Database associates Kawasaki Disease, aka Mucocutaneous Lymph Node Syndrome, with Endotoxin hits on CD40, FCGR2A and ITPKC genes.
https://ctdbase.org/detail.go?type=relationship&chemAcc=D008070&diseaseAcc=MESH%3AD009080&view=reference
I have one triple-jabbed friend who developped quite bad vasculitis. Two other triple-jabbed people had blood clots. One of them had a blood clot three days after the 2nd as well as a larger blood clot three days after the 3rd Pfizer/Biontech injection, the other one needed surgery due to a blood clot after his three Pfizer injections. The blood clot was all the length of his leg. My sister told me that one of her aquaintances, triple-jabbed and 40 years of age, needed an emergency operation due to a blood clot in his leg. The stitches looked ghastly. Obviously the ER doctors had to cut in a great hurry and crudely in order to save his leg from dying. Since they did the emergency operation a couple of hours too late, his leg has now a permanent damage, and he will not be able to get his strength back in that leg. Another friend who had already an autoimmune rheumatic disease with vein problems before Covid seems to have not benefited from her three Covid-injections. Her autoimmune disease got worse, she started having trouble walking with muscle pains in her legs, later after falling down and hitting her head, they gave her epileptic medicines, later she had a wound in her foot that would not heal, I also remember making pictures of her upper legs (it looks a bit like vasculitis or like lupus) later they put stents in her leg because there was a problem with blood circulation, then they had to amputate her leg above her knee becauses the blood circulation was lacking. I personally believe that her three Pfizer injections may have accelerated her autoimmune disease.
I believe that none of the aforementioned conditions were reported to any vaccine adverse effect reporting systems